
Nalin Karunaratne presents a recent case-study.
My patient was a 62-year-old lady with Parkinson’s disease. She also had emphysema and osteoarthritis. This lady was referred from another local practice as she had been suffering from pain and food packing on her lower-left side for the best part of a year, with no solution having been found. She had been to see a dentist who had advised extracting all three teeth, but, seeking a second opinion, the patient was initially referred to our implant surgeon.
A periapical radiograph (fig 1) indicated large distal cervical radiolucencies involving the pulp on LL5, 6 and 7. On the LL6 it extended into the furcation.
Our implant surgeon and I first considered a fixed conventional bridge between the LL5 and LL7, accepting that LL6 could not be saved. However, the prognosis of a bridge in a high-loading area, in a patient with established toothwear from grinding due to stress on two root-treated abutments, was guarded at best.
The patient did not want a denture. Therefore, we decided to try urgently root-treating the LL5 and LL7, with the LL6 being replaced with an implant thereafter.
The patient’s Parkinson’s disease was well controlled and she had full capacity to consent. Everything was explained verbally and a written explanation and summaries were provided and signed, making for robust informed consent.
Treatment pathway
The first objective of the treatment, after a full examination was to root-treat the LL5 and LL7. Due to the long-standing infection and the clinical burden of treating two teeth, we decided this would be tackled in two long visits.
First, I gained access. A rubber dam was used to isolate both teeth. After full caries removal, there was still enough coronal tooth substance left to support two crowns. This would not be straightforward, however, given the extent of carious breakdown.
The LL7 was the more decayed of the two teeth, so to successfully isolate this with the rubber dam was more challenging. Therefore, a gingiva approaching clamp was selected alongside a ‘wash’ impression material to gain the best possible seal.
The LL5 presented with a single canal as expected and the LL7 had two mesial canals and one distal canal. Patency was established with a size 10 K-File. Copious irrigation was carried out with Parcan solution (three per cent sodium hypochlorite) between instruments, with regular recapitulation using the K-File ensuring that the canals were not blocked.
Since they were not particularly narrow in diameter, canal preparation was carried out with the Coltene HyFlex EDM OneFile of ISO 25 apical size, using Canal+ as lubrication.
Using an electronic apex locator it was found that LL5 had a 23mm working length. For the LL7, the distal canal was 19.5mm, the mesiolingual canal was 21.5mm and the mesiobuccal canal 21mm.
At the following visit, obturation was completed with bespoke master apical cones, Roeko Guttapercha Points (ISO size 25), to a good radiographic finish after drying the canals with the corresponding Roeko Paper Points.
We elected to protect the teeth as soon as possible, so cuspal coverage definitive restoration was started straight away.
The LL5 was restored with an e-max onlay, bonded with Coltene Brilliant EverGlow universal composite and the LL7 was restored with a full gold crown, cemented with conventional glass-ionomer cement. The LL6 was deemed to be unrestorable, so it was extracted and replaced with an implant by our implant surgeon.
Outcome
The patient was delighted with the result, which can be shown on the radiograph (Fig 2). She was very grateful to both clinicians, as she could now eat, drink and function without pain.
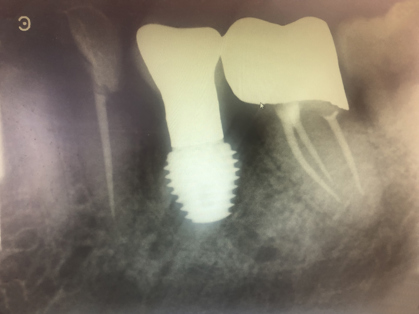
Fig 1.

Fig 2.